The Operational Crutch of the Healthcare Revenue Cycle
Prior authorization (PA) has long stood as one of the most severe operational bottlenecks in the United States healthcare ecosystem. Designed by payers to control costs and ensure medical necessity, the traditional manual PA process—characterized by fragmented faxes, phone queues, and disconnected web portals—has instead introduced profound systemic friction. For medical groups and health systems, this friction converts directly into administrative overhead, severe revenue cycle delays, and extended clinical care-delivery timelines.
However, the regulatory landscape is shifting dramatically. The Centers for Medicare & Medicaid Services (CMS) finalized the landmark Interoperability and Prior Authorization Final Rule (CMS-0057-F), setting off a phased rollout that alters the operational dynamics between providers and payers. This regulatory shift presents a clear choice for healthcare leaders: treat these automation rules as a reactive compliance check, or leverage them as a strategic mechanism to clear revenue cycle friction and accelerate clinical delivery.

Breaking Down the CMS Mandates and Timelines
The CMS-0057-F rule directly regulates impacted payers—including Medicare Advantage (MA) organizations, state Medicaid and CHIP fee-for-service programs, Medicaid managed care plans, and Qualified Health Plan (QHP) issuers on Federally Facilitated Exchanges. While providers are not the direct targets of the mandates, their administrative workflows are heavily impacted by the downstream benefits of these two critical regulatory horizons:
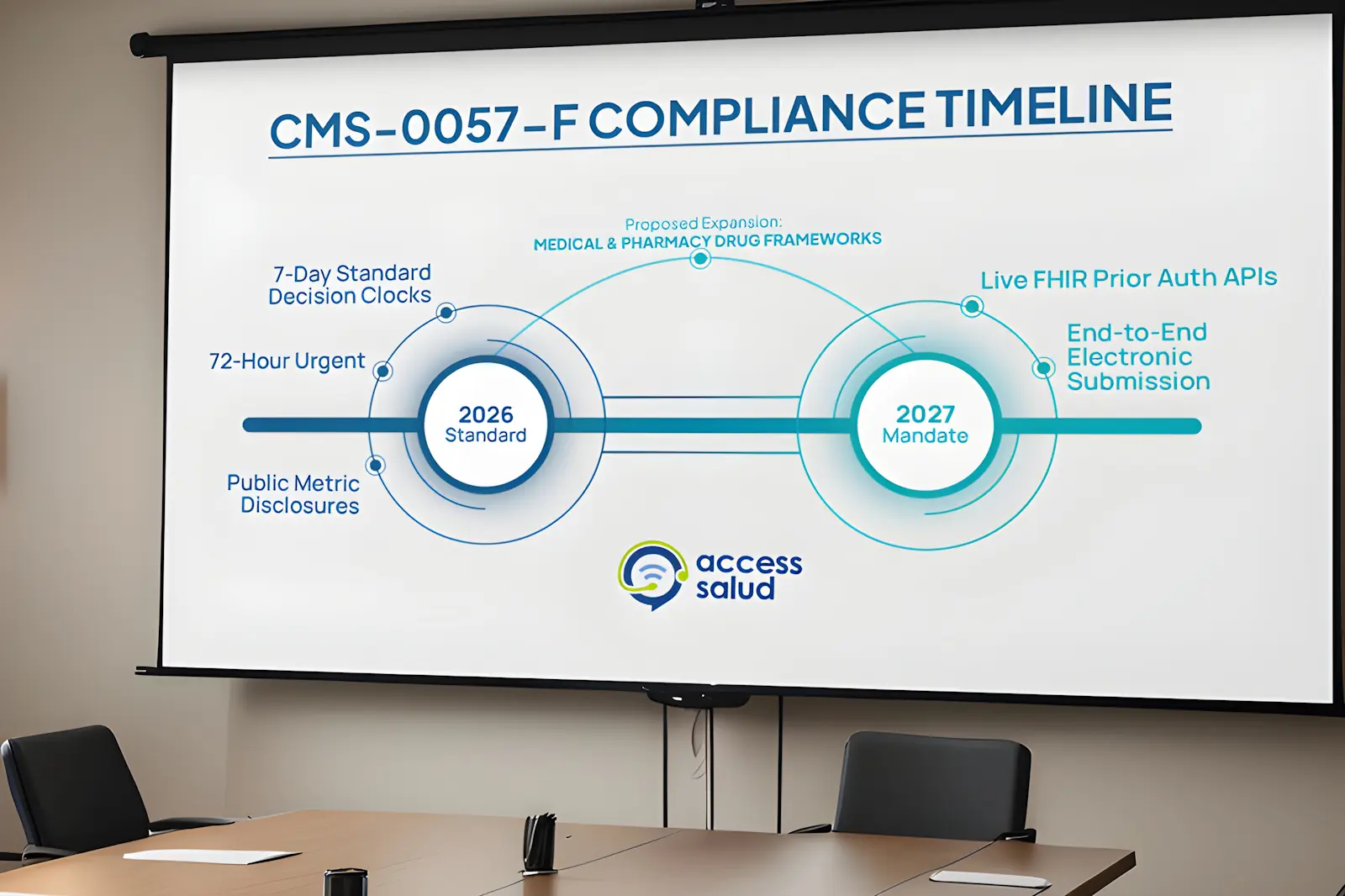
- The 2026 Operational Performance Standards: Impacted payers were required to enforce strict decision timelines: a maximum of 72 hours for urgent/expedited requests and 7 calendar days for standard requests. Additionally, payers must provide specific, structured, and actionable reasons for any prior authorization denial, eliminating vague rejection notices. Payers also faced a public disclosure deadline requiring them to publish initial prior authorization metrics—such as aggregate approval and denial rates—on their public websites.
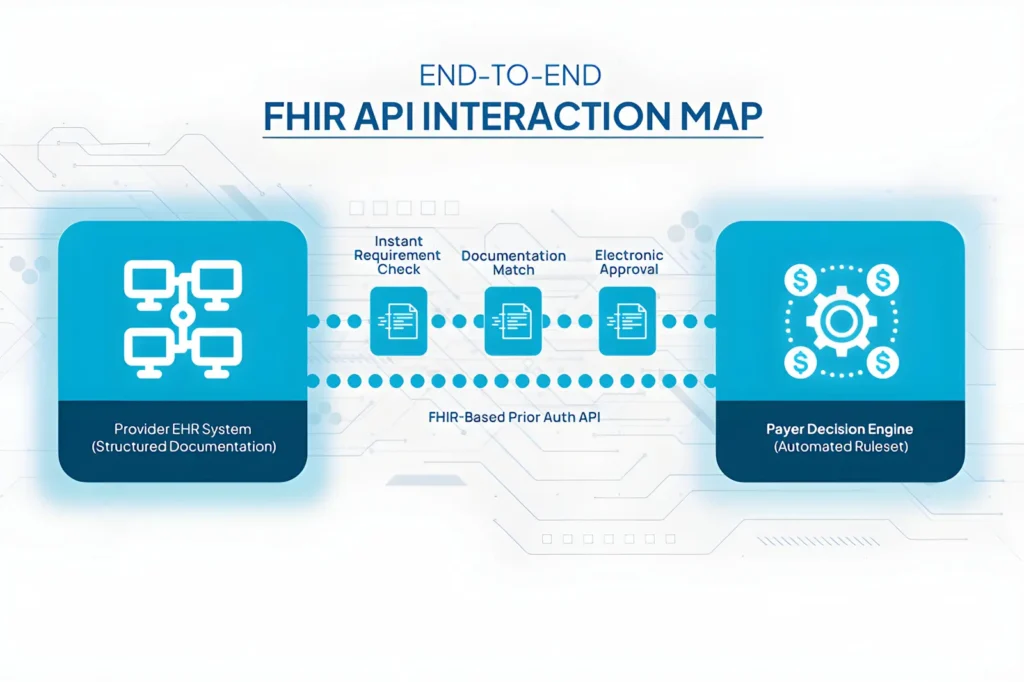
- The 2027 Interoperability API Mandate: Payers must fully implement live, electronic Fast Healthcare Interoperability Resources (FHIR)-based APIs. The core architecture includes a dedicated Prior Authorization API that automates the determination of PA requirements by service, provides explicit visibility into required documentation, and supports end-to-end electronic submission and decisions.
- The New Horizon for Pharmaceuticals: Expanding on this momentum, CMS released a new Interoperability Standards and Prior Authorization for Drugs Proposed Rule. This expansion aims to drag drug prior authorizations out of manual siloes and into the same electronic FHIR framework, standardizing data exchange for both medical-benefit and pharmacy-benefit drug coverages.
[Traditional PA Loop – Antiquated]
Manual Intake ──> Multi-Payer Fax Chaos ──> Vague Denials ──> Revenue & Attrition Loss
[CMS-0057-F Framework – Standardized]
EHR Integration ──> FHIR Prior Auth API ──> Accelerated Decision Clock ──> Streamlined Care Delivery
Strategic Optimization: Turning Automation into Clinical Asset Velocity
The introduction of standardized FHIR APIs and shorter decision windows means that providers can move away from un-targeted manual follow-ups. However, the software infrastructure provided by payers is only as effective as the provider’s internal data readiness. To capitalize on electronic prior authorizations, healthcare organizations must systematically audit their clinical documentation workflows.
Because payers must supply explicit rejection metrics, revenue cycle teams can utilize advanced analytics to map denial trends by procedure code, payer type, and documentation gap. When an optimized patient access team manages this automated pipeline, clinical information can be structured correctly at the point of intake. This data precision ensures that when electronic requests are pushed through the payer’s API, they are verified as “complete” on the first pass—minimizing back-and-forth communication, protecting provider utilization rates, and mitigating the administrative fatigue that frequently drives staff burnout.
Conclusion: Cultivating Structural Efficiency in a Regulated Market
Navigating the evolving CMS Interoperability mandates requires an operational framework that matches technical software rules with disciplined execution. Organizations that rely on legacy, manual authorization processes risk falling behind as payers transition to highly automated, algorithmic decision models.
By restructuring patient intake, aligning clinical documentation with standardized data elements, and actively monitoring payer adherence to decision timelines, medical practices can effectively insulate their revenue cycle from structural friction. Embracing these automation rules transforms an administrative hurdle into a measurable competitive advantage that accelerates patient access and secures long-term business continuity
To evaluate how your medical practice or health system can reengineer its patient access workflows to fully exploit the new CMS electronic prior authorization frameworks, contact us today to schedule an operational assessment with our Management Team.



