The New Operational Standard for Health Equity
For population health managers, compliance officers, and hospital executives, tracking Social Determinants of Health (SDOH) has evolved from an idealistic clinical objective into a strict regulatory mandate. Following voluntary reporting phases, the Centers for Medicare & Medicaid Services (CMS) is making standardized SDOH reporting mandatory in 2026. Health networks must now systematically screen patients for Health-Related Social Needs (HRSNs), specifically targeting food insecurity, housing instability, transportation barriers, and utility difficulties.
While the clinical value of addressing these non-medical drivers of health is indisputable, the administrative reality is daunting. Capturing, structuring, and acting upon this highly qualitative data introduces massive operational friction. Without a dedicated strategy, the SDOH mandate threatens to become an overwhelming clerical burden that bogs down frontline staff and lengthens patient intake cycles.
The Z-Code Bottleneck: Quantifying the Data Collection Gap
Operationalizing SDOH data relies heavily on the accurate implementation of ICD-10-CM codes—specifically categories Z55 through Z65, commonly known as “Z-codes,” which identify socioeconomic and psychosocial risks.
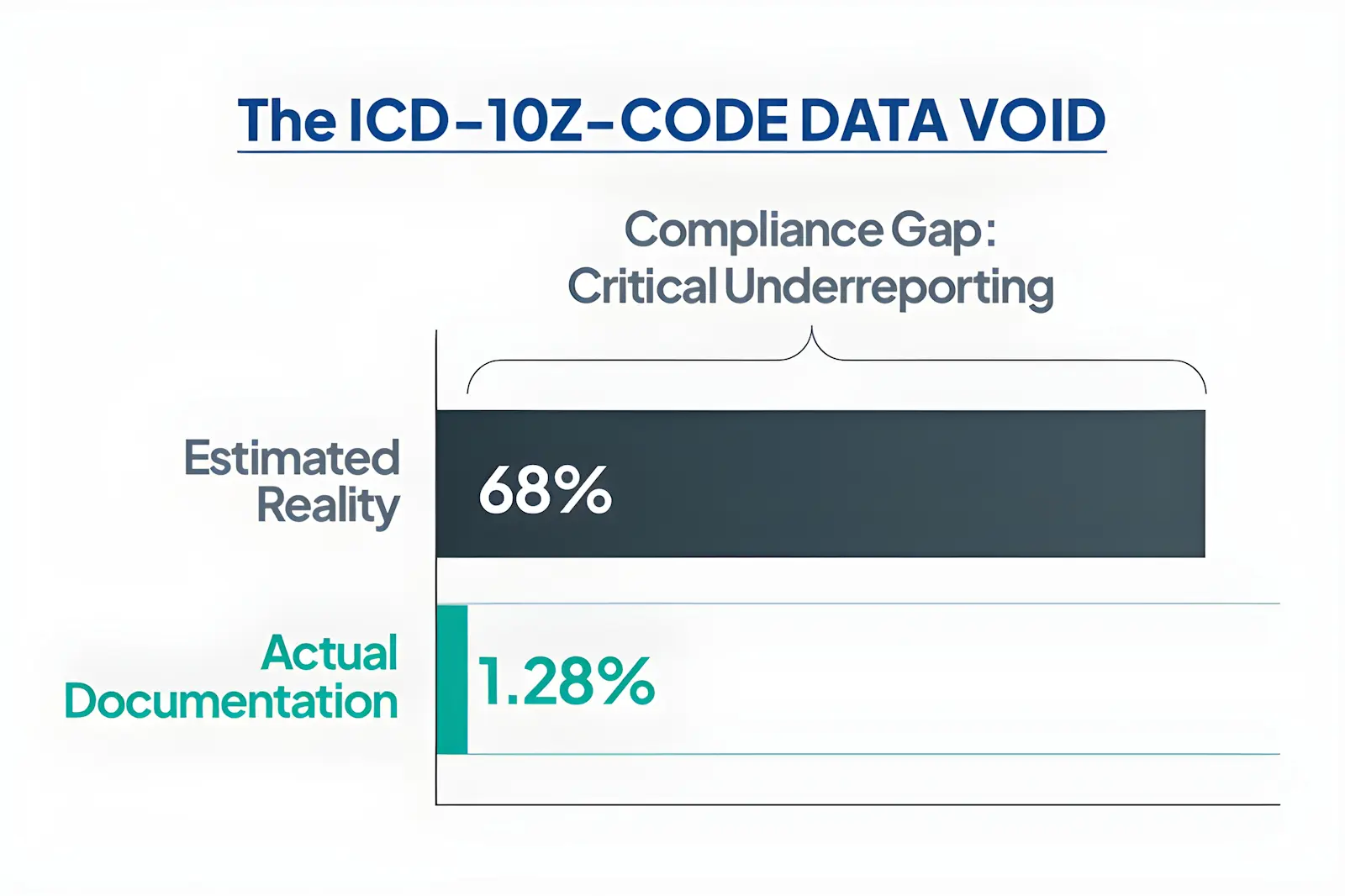
Despite the availability of these codes, healthcare systems are failing to capture the data. According to the American Hospital Association (AHA), historical CMS data showed health care providers used Z-codes for a mere 1.6% of Medicare fee-for-service beneficiaries. More recent industry analyses reveal that even within expansive datasets of over 1.4 million patients, Z-codes are documented for just 1.28% of the patient cohort—an alarmingly low capture rate considering estimates suggest up to 68% of patients are impacted by at least one social factor.
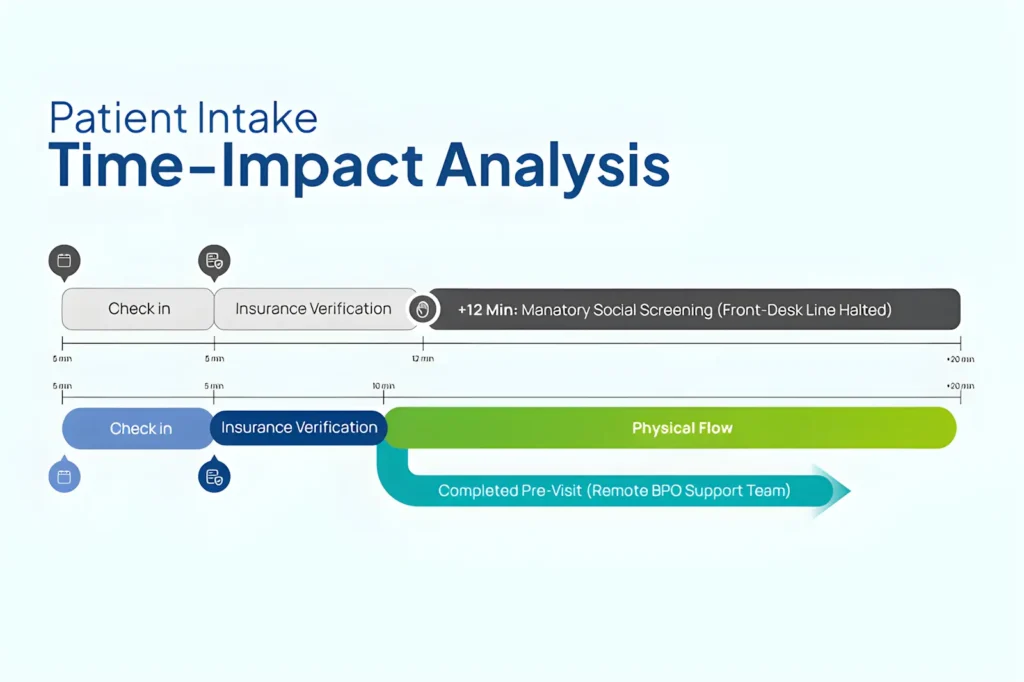
The primary barrier to compliance is clinic time. Frontline medical assistants and receptionists, already buried under insurance verification and prior authorizations, do not have the capacity to navigate these sensitive conversations during standard check-in. Consequently, screenings are either rushed, skipped entirely, or documented as unstructured free text within the Electronic Health Record (EHR).
[The Broken SDOH Flow]
Raw Intake ──> Rushed Screening ──> Unstructured Text Note ──> Zero Z-Code Billing ──> Missing VBC Incentives
[The Operationalized SDOH Flow]
Outsourced Pre-Visit ──> Structured Screening ──> Automated Z-Coding ──> Closed-Loop Referral ──> Maximize Quality Metrics
Moving Beyond Capture: Closing the Loop on Social Care
Collecting the data is only the first half of the mandate; the true operational challenge lies in executing closed-loop referrals.
When a screening flags a patient for food insecurity or lack of medical transportation, the practice must have an established workflow to connect that individual to local community resources. Under the National Committee for Quality Assurance (NCQA) Social Need Screening and Intervention (SNS-E) HEDIS measure, simply asking the question is not enough to satisfy quality metrics. To meet the measure, a corresponding intervention—such as a referral, assistance, or coordination—must be provided and documented within one month of a positive screen.
Managing this ongoing outreach requires a continuous administrative effort that physical, clinic-based teams cannot sustain without neglecting their immediate, in-office clinical duties.

The Solution: Scaling Population Health via Specialized BPO Support
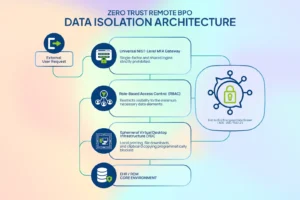
To master the SDOH mandate without compromising clinical efficiency, forward-thinking healthcare networks are decoupling social screening from the physical clinic floor. By shifting this workflow to an outsourced, specialized care management support team, the entire data lifecycle is optimized.
Operating as an extension of your practice, remote care coordinators can conduct structured, empathetic bilingual screenings via phone or patient portal prior to the scheduled appointment. These specialists accurately log the appropriate ICD-10 Z-codes directly into the practice’s EHR, trigger automated referrals to community resources, and manage the extensive 30-day follow-up required to close the loop. Integrating this off-floor workflow support allows practices to drastically scale data capture without adding a single administrative task to physical clinical providers.
Operationalizing SDOH data is no longer an administrative luxury—it is a core requirement for modern healthcare delivery. By implementing a systematic, outsourced framework to absorb the screening and referral workload, clinical leaders can bridge the gap between compliance and care.
When you build a structured infrastructure to manage social needs, you execute a strategy rooted in spatial empathy—designing workflows that respect the physical boundaries and capacities of your in-house staff while still delivering true, comprehensive health equity to the communities you serve. To evaluate how your organization can seamlessly scale these workflows without compromising internal capacity, contact us today to schedule an assessment with our Management Team and explore strategic partnership opportunities.